

SADI- S surgery, introduced in medical literature by Dr. Scorpinaro, is a surgical method in bariatric surgery that has been safely applied in the USA for 20 years and it is an alternative method in bariatric surgery as “duodenal switch and biliopancreatic diversion” has numerous metabolic effects. Having almost the same effects as “Duodenal Switch” surgery, SADI – S (Single anastomose Duodeono – Ileal Bypass with Sleeve Gastrectomy) may be regarded as less riskier surgical method as it involves single anastomose (Gastrointestinal connection).
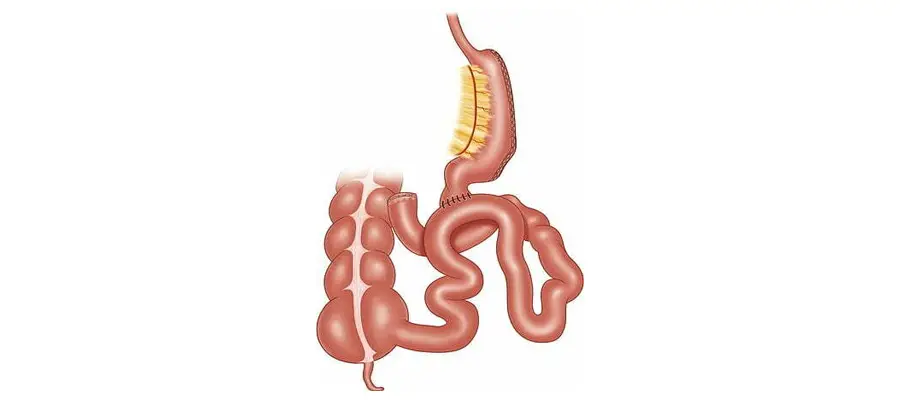
In this surgical method, firstly classic gastrectomy is performed. Then small intestines that are approximately 5-6 meters in length and whose main duty in our body is nutrient absorption are bypassed therefore absorption area is cut down to 2.5 meters. There is no removal of intestines from the body during this operation. The method focuses on reducing contact area of nutrients, the remaining intestines continue assisting normal bile and pancreas flow.
This procedure is restrictive as it involves gastrectomy and it is also malabsorptive as it involves bypass. In addition to reduction of absorption, it triggers production of a hormone called GLP-1 in small intestines that stimulates satiety center. This results in significant reduction in appetite. It’s important to note that “psychological hunger” also has a role in appetite. If the patient has an eating disorder and it is not treated with psychoanalytic methods, there may be a relapse in weight gain in the long term.
The most distinguished feature of SADI-S method is the preservation of pyloric stenosis that regulates the outflow of nutrients into duodenum and prevent “Dumping Syndrome” which is one of the most feared complication of bypass surgeries. Dumping Syndrome generally occurs when the patient is eating a meal or after 10 minutes after they have finished eating and it slows down in about 40-60 minutes.
It is often experienced when the patient is still seated during a meal. Vasomotor symptoms are common and sometimes it may deactivate gastrointestinal symptoms. Patients often experience fatigue, dizziness and fainting and they feel the urge to lay down. They complain about cold sweats and palpitation along with satiety and nausea in the stomach.
It is vital to be able to endoscopically view all parts of stomach especially for those who are in stomach cancer risk group and with a family history of stomach cancer. In Roux-n-y gastric bypass and mini-gastric bypass methods, there are parts of stomach that cannot be viewed endoscopically but this does not go for SADI-S surgery.
In this method, regulation of glucose is more successful compared to other methods in especially patients with glucose problems.